Who Benefits When Nurse Practitioners Gain Independence? Patient Sorting, Disease Detection, and Health Outcomes
The United States faces a growing primary care crisis. Long wait times and provider shortages prevent millions of Americans from receiving timely care. To close this gap, healthcare systems have increasingly turned to nurse practitioners (NPs), registered nurses with advanced training who can diagnose illnesses, order tests, and prescribe medications. NPs now nearly outnumber physicians and are growing at an even faster rate, and their role in primary care has grown rapidly over the past decade. By 2022, 30 states had granted NPs rights to practice without physician supervision.
Yet a debate persists: should NPs be allowed to practice independently, without physician oversight? This paper provides new and comprehensive evidence on what happens when they do: how the policy reshapes which patients see NPs, how it affects the detection of chronic diseases, and whether it changes the quality of clinical care. This paper is the first to investigate how patients sort into physicians and NPs and to examine NP care relative to that of physicians.
Finding 1. NP autonomy expands access for the highest-risk patients
My first finding on patient sorting is that following the adoption of full NP practice authority, patients with three or more pre-existing chronic conditions increase their annual NP visits by 0.29 visits over four years—a remarkable 46 percent increase relative to their baseline utilization. These same patients modestly reduce their visits to primary care physicians. Healthier individuals with fewer chronic conditions show no significant change in their provider choices. This is a novel and important finding: when NPs gain independence, it is the sickest patients—not the healthiest—who take advantage of expanded access.
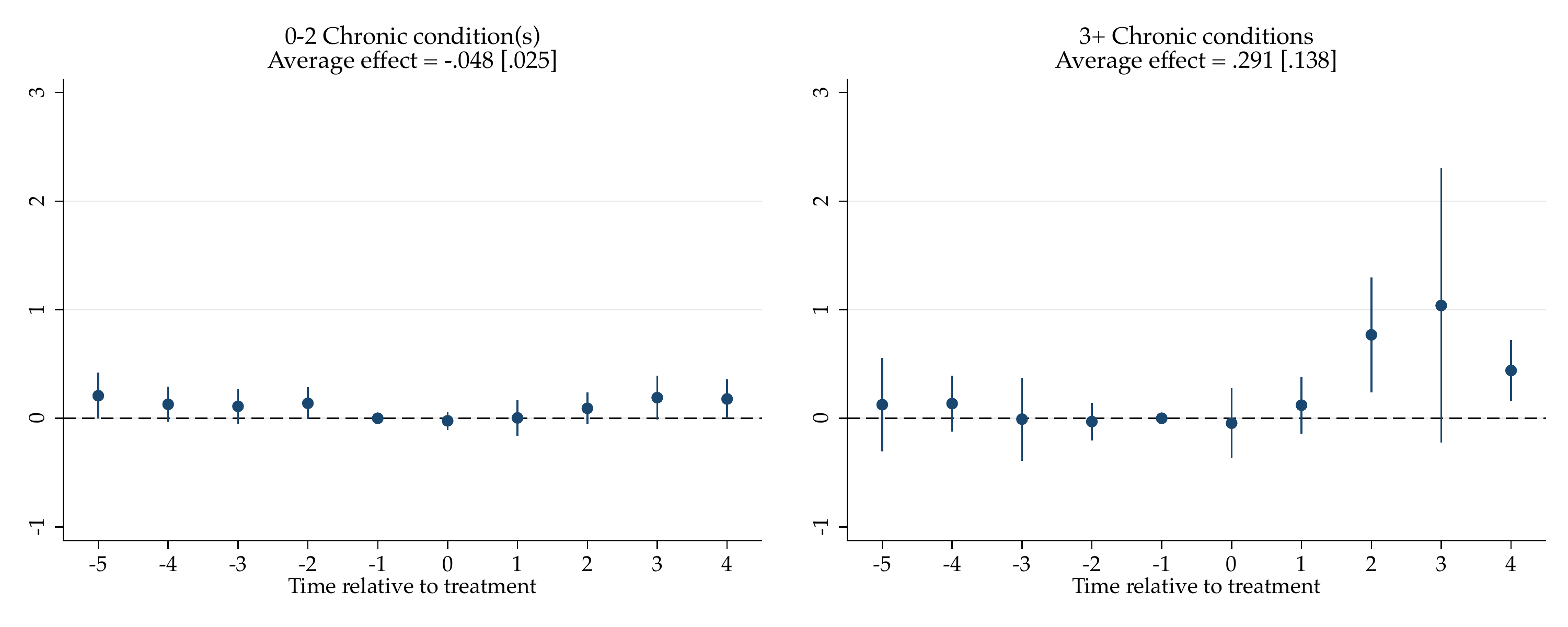 The figure shows the effects of state-level NP full practice authority on annual NP visits by patients’ pre-reform chronic conditions. Point estimates with 90% confidence intervals are reported by treatment year.
The figure shows the effects of state-level NP full practice authority on annual NP visits by patients’ pre-reform chronic conditions. Point estimates with 90% confidence intervals are reported by treatment year.
Finding 2. NP autonomy uncovers hidden diseases without improving health scores
The second finding is that diagnoses of major chronic conditions increase substantially following NP autonomy. Among individuals with fewer pre-existing conditions, the probability of being newly diagnosed with high blood pressure rises by 3.4 percentage points and arthritis by 3.1 percentage points. The effects are even larger among higher-risk individuals. These findings suggest previously undiagnosed conditions are being identified after the policy.
Health measures do not improve. The Physical Component Summary (PCS) score—a standardized measure of physical health—decreases by about 0.6 points annually among both lower-risk and higher-risk individuals, although these changes fall below thresholds for clinical significance. Emergency room visits show a modest increase among higher-risk patients.
Finding 3. NPs expand their prescribing role after gaining autonomy
At the visit level, the paper reveals important changes in NPs’ clinical activities. Full-practice NPs prescribe more medications than their restricted-practice counterparts: when a patient visits a full-practice NP, the probability of receiving any prescription is 3.9 percentage points higher. Central nervous system agents—including analgesics and anti-inflammatory drugs for pain management—account for roughly 40 percent of this increase, with prescriptions rising by 1.7 percentage points. Psychotherapeutic agents increase by 1.0 percentage point and cardiovascular medications by 1.8 percentage points. These patterns reflect NPs taking on a broader clinical role, particularly in managing chronic pain, mental health conditions, and cardiovascular diseases.
Policy Takeaways
I provide the first evidence that NP autonomy triggers selective patient sorting based on health risk, with the most medically complex patients driving the increase in NP utilization. I demonstrate that expanded NP access detects substantially more chronic diseases—a critical first step toward better disease management and reduced long-term healthcare costs. I also show that NPs maintain diagnostic standards and increase prescriptions.
However, there is no compelling evidence that health measures improve, including self-reported health and critical health events. To better understand why health status shifts little after the policy, future research incorporating detailed information on clinical decision making (e.g. interpretation of diagnostic measures, prescription adherence) and longer-term health data will be essential. As NPs become an ever-larger share of primary care providers, understanding the consequences of their expanded autonomy is crucial.
The full paper is available on my Research page.